
Distal radius fracture types seen in the hand therapy clinic
Filed under Evaluation
Distal radius fractures are one of the most common injuries seen in hand therapy. Several different distal radius fracture classification systems have been developed, and this blog post will focus on the more common types of distal radius fractures and their classification.
Extra-articular fractures are either nondisplaced or displaced fractures. These fractures occur outside of the joint.
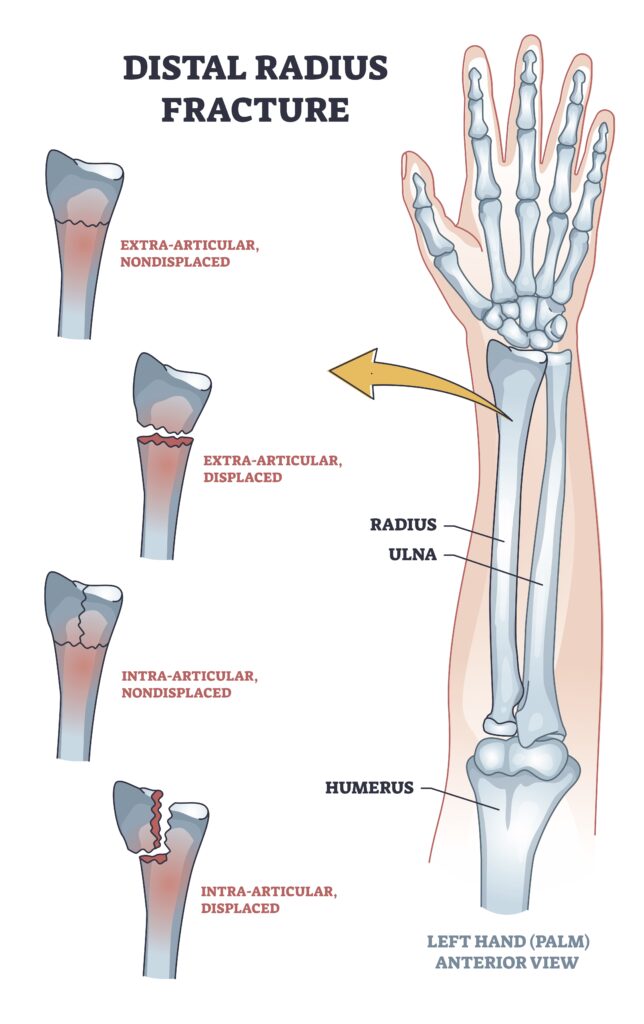
Similarly, Intra-articular fractures can be displaced or nondisplaced but occur within the joint.
Many fractures are named based on their fracture location, fracture pattern, and type of displacement.
Colles fractures are the most common type of distal radius fracture and account for about 90% of distal radius fractures. A Colles fracture is an extra-articular fracture with a dorsal displacement. These fractures occur from a fall forward on an outstretched hand.
A reverse Colles fracture is also known as Smith’s fracture. This is also an extra-articular fracture that is volarly displaced. These types of fractures are caused by falling backward and an outstretched arm.
Another type of distal radius fracture is a Barton’s fracture. This is an intra-articular fracture and is associated with a dislocation of the radio-carpal joint. A Barton’s fracture can be described as volar (more common) or dorsal (less common).
A die punch fracture is a depression fracture of the lunate fossa of the distal radius fracture that occurs with a vertical load through the lunate. These are often overlooked and not part of the classification system.
A Chauffeur’s fracture is also known as a radial styloid fracture or a Hutchinson’s fracture. This fracture is classified as an articular fracture. It was initially called a Chauffeur’s fracture because when the chauffeur would turn the crank to start the car, the motor often would cause the crank handle to jerk back.
1 Comment
Leave a Comment
More To Read

Sensitivity and Specificity in Thoracic Outlet Syndrome (TOS) Tests in Hand Therapy
By: Mikayla Murphy Sensitivity and Specificity in Thoracic Outlet Syndrome (TOS) Tests in Hand Therapy Thoracic outlet syndrome (TOS) describes the compression of nerves, arteries, and veins as they pass through the thoracic outlet. Compression can occur at the interscalene triangle, the costoclavicular triangle, and the subcoracoid space (Physiopedia, n.d.). There are three types of…

Do you know the difference between an Electromyography (EMG) and a Nerve Conduction Velocity (NCV) Study?
Do you know the difference between EMG and NCV (an Electromyography and a Nerve Conduction Velocity Study? The term nerve test is usually a broad term that typically indicates both an Electromyography (EMG) and a Nerve Conduction Velocity (NCV) study (EMG vs NCV). An EMG looks at the electrical signals your muscle makes when at…

Dorsal Wrist Pain?
Incorporating Emerging Evidence into Clinical Practice for Patients Experiencing Dorsal Wrist Pain During Weight-Bearing Activities By: Brittany Day Supporting Evidence A randomized control study recently published in the Journal of Hand Therapy found rigid carpal stabilizing taping (CST) to significantly increase passive range of motion, active range of motion, and decrease pain in patients experiencing…

Trigger Finger… Quick and Dirty!
This is for you… Hand Therapists! Stenosing tenosynovitis, otherwise known as trigger finger, is a common condition affecting children and adults of all ages. Fast Facts Trigger finger usually occurs at the A1 pulley It occurs with inflammation of the tendons and sheaths of fds and fdp The digit can lock in both flexion and…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
Thank you so much! I always enjoy your informative blogs and have learned a great deal. Your effort is very much appreciated!!!