
Brachial Plexopathy Case Example in Hand Therapy (plexopathy examples)
One of the recent cases we have seen is a 13-year old with a brachial plexus injury. We are seeing the patient post-surgery for tendon transfers to increase functional use of his left upper extremity (LUE).
Before the surgery, he could not extend the wrist and fingers to even hold his hand in a neutral position due to ulnar and radial nerve entrapment involvement. As a result, the surgeon transferred flexor carpi radialis (FCR) to extensor digitorum communis (EDC), palmaris longus (PL), to extensor pollicis longus (EPL), pronator teres (PT) to extensor carpi radialis brevis (ECRB). Next, a babysitter transfer was performed for the ulnar sensory nerve to the median nerve and the hand level.
The patient began therapy 7.5 weeks after surgery to begin activation of transferred tendons for improved functional extension of wrist and hand. The patient presented with trace motion to D1-D4 with a MMT of 2-/5 for the new EDC. The small finger is not active and was not included in the EDC transfer due to the small size. The patient had slight flexion to transfer foam cubes using IF and thumb. However, weakness in wrist and digit extensors in combination with flexor transfers causes difficulty with active flexion. As a result, in therapy sessions, we are focusing on small functional motions of the fingers and with wrist stabilization and endurance of the shoulder/
Explicit Therapeutic Exercise Interventions
- In order to activate the FCR that is now the EDC and the PT that is now the ECRB, the forearm is isolated with the right hand. Radial deviation is blocked at the radial border of the 2nd metacarpal in order to perform wrist extension in a uniplanar motion. Repetitions are completed about 10 times for 3-4 sets depending on patient fatigue.
- For PL to EPL activation, formation of a pincer grasp with thumb extension between repetitions is used to transfer foam cubes, not only working on thumb extension, but also intrinsic opposition with opponens pollicis and abductor pollicis brevis. Within this activity, the focus is on making a neat circle with the thumb and opposing finger in order to increase intrinsic stability rather than collapsing at the thumb, to make this a more functional grasp pattern for future tasks.
- Ball rolling while maintaining palm and digit contact rolling the ball in a sagittal plane for proximal stability and to increase wrist flexion and extension pattern with PROM for proprioceptive feedback and motor memory.
Functional Therapeutic Activities
- Placing foam cubes into an egg crate for increased wrist extension while maintaining pincer formation.
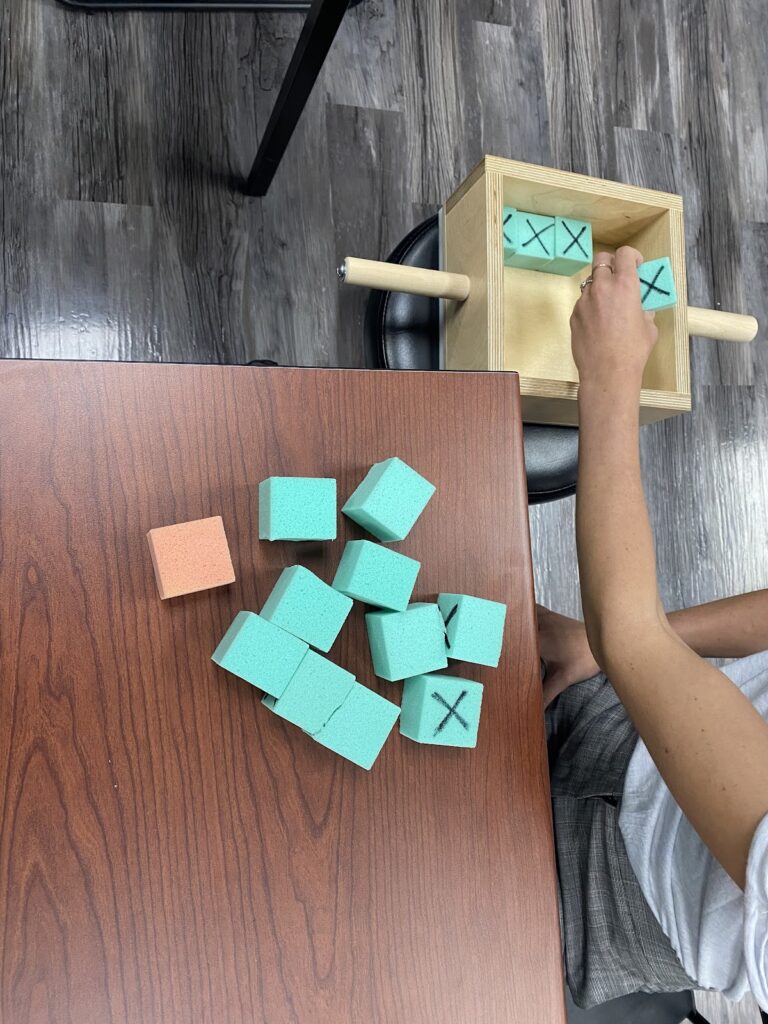
- Transfer large foam cubes with a black “X” on one side, from the table to a 1’x1’ box on a lower surface next to the patient, and then organize the blocks so that the black X is facing up. The block fits into the box with only a little space left, making the task challenging due to the planning and precision required to place the blocks in a uniform manner. This activity is performed to work on motor planning and UE endurance.
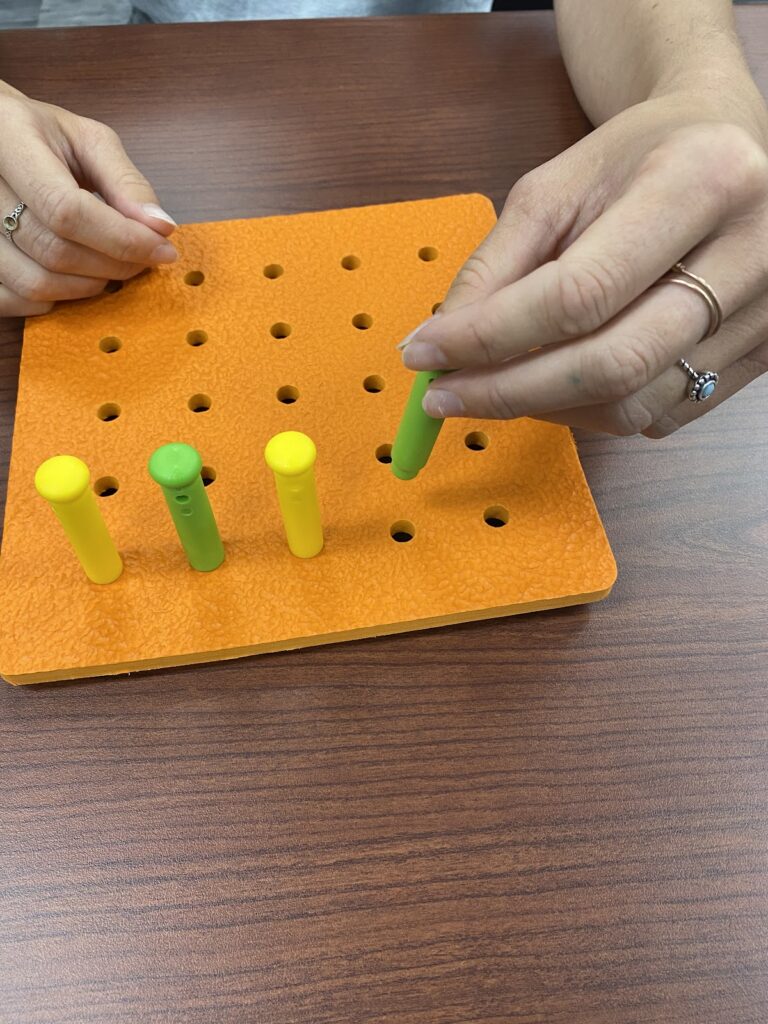
- Built-up pegboard with a wider grip for tripod grasp formation. This activity requires the patient to obtain a secure grip on the peg to place into the board and work on accuracy and proximal stability of the shoulder and elbow. The patient demonstrates weakness to the shoulder due to lack of use, which has been an unforeseen challenge to many activities, causing fatigue to not only the hand and wrist but the whole arm.
The patient has been making good progress overall. He still requires the forearm to be supported to acquire and maintain a pincer grasp, but his 1st webspace stability is improving. Shoulder fatigue continues to be a problem, and the patient continues to require a lot of rest breaks. The patient is learning to balance activities evenly not to overtax the shoulder.
More To Read
Hand Therapy: Does Dry Needling work to Treat Trigger Finger
By: Taylor Volentine Reference: Azizian, M., Bagheri, H., Olyaei, G., Shadmeher, A., Okhovatpour, M. A., Dehghan, P., Jalaei, S., Sarafraz, H. (2019). Effects of dry needling on tendon-pulley architecture, pain and hand function in patients with trigger finger: a randomized controlled trial study. The Journal of Physical Therapy Science, 31. 295-298. doi:10.1589/jpts.31.295 Photo retrieved from…
Read More
5+ Common Mallet Finger Splints
Finger orthoses can be tough, and the mallet finger orthosis is no exception. The protocol for 15 degrees of DIP extension with mallet fingers is tricky to manage while making a splint. Small splints on little fingers are also tricky to get sized just right and with strapping in the right places. Ask any experienced…
Read More
How To Do A Fast but Thorough Hand Therapy Assessment
We don’t get a lot of time. Sometimes new patients come in unexpectedly or someone comes at the wrong time and your 1-hour block for an eval is suddenly only 30 minutes. Do you know how to get the most out of your eval time with the patient? Do you know what things are the…
Read More
Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.