
Scapholunate Wrist Injuries in Hand Therapy
In outpatient hand therapy, we get a variety of referrals ranging from post-operative patients to those looking to avoid or prolong surgery. These referrals come from a variety of sources ranging from primary care doctors to experienced hand surgeons. The therapy orders can be vague to very specific.
One of the more difficult referrals to get is the vague therapy order that states “wrist sprain” or “wrist pain”. These orders require careful evaluation and consideration to prevent further injury and to appropriately treat.
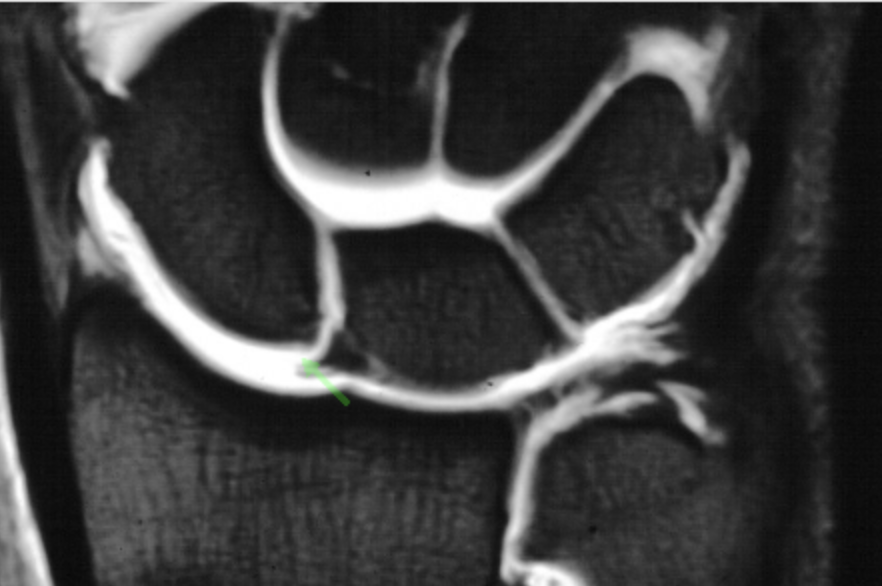
Recently a patient was sent to hand therapy by his primary care doctor after developing worsening wrist pain. The patient is a 59-year male who was playing golf when he hit the ground with his club, sustaining a wrist injury in May of 2021. The patient was sent to traditional physical therapy for wrist pain. During this period of therapy, he did wrist extension/flexion with weights for strengthening of extensor carpi ulnaris (ECU) and flexor carpi radials (FCR/FCU), along with weight-bearing scapholunate instability exercises. His symptoms worsened and his strength significantly decreased. When his symptoms did not improve he sought out a hand surgeon. He underwent an arthroscopic examination where it was found that he had chronic scapholunate (SL) injury to the dorsal ligament.
The patient was then sent to hand therapy for conservative treatment.
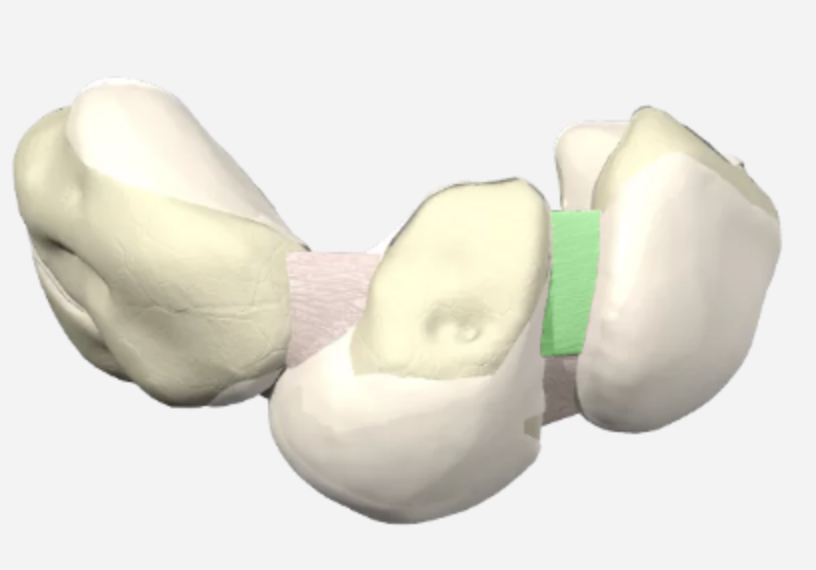
In the previous, therapy session, the patient was performing repetitive ECU and FCR strengthening using weights along with weight-bearing exercises that actually caused the symptoms to worsen (wrist instability exercises). The ECU is a carpal pronator, performing repetitive strengthening of this muscle places additional stress on the SL ligament and cause the SL gap to widen. The Flexor carpi radialis (FCR) muscle is known to have a dual role in wrist stability. It can promote both supination and pronation of the scaphoid and triquetral bones. Initiating strengthening of the FCR muscle should be done with care and based on the extent of injury to the SL.
Scapholunate-friendly strengthening muscles are those that pull the scaphoid into supination and stabilize the SL joint. These include the ECRL, wrist extension and radial deviation, FCU-wrist flexion and ulnar deviation, APL-thumb abduction. The FCR muscle can be a friendly and unfriendly carpal stabilizer, depending on the stage of SL injury. With complete SL injuries, cadaver studies show a significant increase in the movement arm of the FCR, showing strengthening scapholunate instability exercises would be detrimental and lead to further SL instability.
Proprioceptive exercises are an important part of the rehabilitation process for SL injuries as well. The neuromuscular stabilization of the SL with the use of proprioception has been shown to improve dynamic carpal stability. Proprioceptive exercise can range in difficulty from tossing a tennis ball to using a proprioceptive disc stacker to using a gyroscope.
After advancing the presented patient through SL stabilization exercises and proprioceptive exercises for 8 weeks. The patient has decreased complaints of pain, improved range of motion, and was able to return to work with a pain-free wrist. Knowing the etiology of wrist pain is crucial to providing the appropriate treatment.
References
Hagert, Elisabet (2010). Proprioception of the wrist joint: A review of current concepts and possible implication on the rehabilitation of the wrist. Journal of Hand Therapy, 23, 2-17.
Salva-Coll, G., Garcia-Elias, M., :& Hagert, E. (2013). Scapholunate instability. Journal of Wrist Surgery, 2, 136-140.
1 Comments
Leave a Comment
More To Read

Hand Therapy Article Review: The Radial Synergy Test, An Aid to Diagnose de Quervain’s Tenosynovitis
Chihua, L., Langford, P.N., Sullivan, G.E., Langford, M.A., Hogan, C.J., & Ruland, R.T. (2021) The radial synergy test: an aid to diagnose de Quervain’s tenosynovitis. HAND. epub ahead of print;1-6. doi: 10.1177/15589447211057297 Rapid Review By: Case Peters The Skinny: de Quervain’s tenosynovitis is a common pathology that involves swelling and thickening of the tendon sheaths…
Read MoreOccupational and Physical Therapy Continuing Education: Evidence‑Based Practice and Research Literacy
Introduction: The Role of Research in Modern Occupational and Physical Therapy In today’s healthcare landscape, staying updated isn’t a luxury—it’s a necessity. As new research floods academic journals and treatment methodologies evolve, therapists must stay ahead. This is where occupational and physical therapy continuing education comes in. More specifically, courses that emphasize evidence-based practice (EBP)…
Read MoreDoes Taking an Alpha-lipoic for 40 days after Carpal Tunnel Release decrease the likelihood of developing Pillar Pain?
Filippo, B., Granchi, D., Roatti, G., Merlini, L., Sabattini, T., & Baldini, N. (2017). Alpha-lipoic acid after median nerve decompression at the carpal tunnel: A randomized controlled trial. The Journal of Hand Surgery, 4, 236–42. The Skinny – A double-blind, randomized controlled study was performed. Sixty-four patients were randomly assigned into two groups after median…
Read More
Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
this article is excellent. At times this patients fall in the wrong hands causing more damage and disability.